 |
Case Report
Ureteral stent migration through colovesical and vesicovaginal fistulas in a patient with stage IV cervical cancer treated with pelvic radiation
1 HCA Healthcare/USF Morsani College of Medicine GME (PGY-1), Department of Internal Medicine, Citrus Memorial Hospital, Inverness, Florida, USA
2 HCA Healthcare/USF Morsani College of Medicine GME (Teaching Faculty), Department of Internal Medicine, Citrus Memorial Hospital, Inverness, Florida, USA
Address correspondence to:
Jennifer Klein
Citrus Memorial Hospital, Department of Internal Medicine-Graduate Medical Education, 502 W Highland Blvd, Inverness, FL 33452,
USA
Message to Corresponding Author
Article ID: 100093Z10JK2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Klein J, Gandhi S. Ureteral stent migration through colovesical and vesicovaginal fistulas in a patient with stage IV cervical cancer treated with pelvic radiation. J Case Rep Images Oncology 2021;7:100093Z10JK2021.ABSTRACT
Introduction: Pelvic radiation is often used as radical treatment or additional therapy in patients with gynecologic malignancies. Irradiation damages deoxyribonucleic acid (DNA) of tumor cells by an inflammatory process with several inciting factors. The inflammatory process continues well after the treatment has been given and its effects can present decades after initial treatment. Complications of radiation are related to tissue damage due to parenchymal and vascular endothelial cell death as well as fibrosis resulting from innate immune response. Fibrosis is a late complication of radiation therapy and can present as stenosis or fistulas. Fistulas have an annual incidence rate of up to 5% and can develop anywhere in the irradiated field.
Case Report: This case describes a patient with vesicovaginal fistula secondary to stage IV cervical cancer treated with pelvic radiation. The patient had ureteral stent placement for radiation-induced ureteral stricture which exited the body through the anus through the vesicovaginal fistula and a colovesical fistula which developed over the course of 10 years after initial treatment with radiation therapy.
Conclusion: As cancer survivorship rates increase with improved treatments, it is important to anticipate continuing radiation damage in patients who have received radiation therapy.
Keywords: Cervical cancer, Pelvic radiation, Radiation-induced ureteral stricture, Ureteral stent, Vesicovaginal fistula
Introduction
Combination chemotherapy and radiation is the standard treatment for cervical cancer International Federation of Gynecology and Obstetrics (FIGO) stages IIb and above [1]. Radiation therapy for the treatment of malignancy is often limited by the constraints of avoiding damage to surrounding normal tissue. Historically, cell death as a result of direct cytotoxicity has explained tissue injury but other mechanisms such as inflammation and innate immune response have been considered recently [2]. Destruction of parenchymal and vascular endothelial cells has been thought to result in the production of reactive oxygen species which causes oxidative damage and the release of pro-inflammatory cytokines. Both the oxidative damage and cytokines cause inflammation and trigger the innate immune response resulting in further parenchymal and vascular endothelial cell death and tissue damage [2]. These processes lead to the development of fistulas, stenosis, and fibrosis of tissue in the irradiated field.
A retrospective review of over 2000 patients treated for cervical cancer over a ten-year period found that about 2% developed fistulas off of which had received pelvic radiation [3]. Other studies and case presentations have reported complications as late as 30 years after initial treatment [1]. Although fistulas are an expected complication of pelvic radiation, fistulas occurring by different etiologies at different time intervals have not been widely described in available literature. This case describes an interesting occurrence resulting from the consequences of metastatic pelvic malignancy and radiation therapy.
Case Report
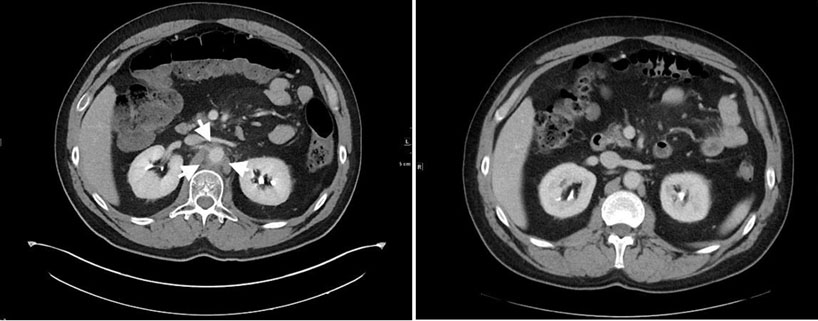
A 55-year-old Caucasian woman presented to the emergency department with complaint of displaced ureteral stent from the anus. She has a history of chronic kidney disease stage IV due to anatomic anomaly of horseshoe kidney with atrophic left kidney as well as vesicovaginal fistula resulting from stage IV cervical cancer treated with high-dose brachytherapy and external beam radiation 10 years ago. Four years after initial treatment with pelvic radiation, she was diagnosed with hydronephrosis secondary to radiation-induced ureteral stricture for which she began to have regular ureteral stent exchanges. The patient presented with the displaced ureteral stent about five years later. The patient said she noticed the end of the stent exiting her anus while she was using the restroom. Urology was consulted which performed cystoscopy to reposition the ureteral stent. The urologist introduced his finger in the rectum to manipulate the stent back into position and was able to visualize the finger on cystoscope which confirmed the diagnosis of colovesical fistula with erosion of the posterior bladder wall (Figure 1 and Figure 2). She was treated with percutaneous nephrostomy catheter placement for ureteral stricture and vesicovaginal fistula as well as a loop colostomy for the colovesical fistula on the same admission. The patient tolerated both procedures well and there were no complications reported.


Discussion
The development of fistulas due to radiation therapy has been shown to occur in 2% of patients within 10 years of initial treatment [1]. Vesicovaginal fistulas are more common in cancer patients with bladder metastasis at the time of diagnosis than as a result of radiation damage and are typically evident about three months after diagnosis of metastatic cervical cancer. Studies have shown that other comorbidities and patient-specific features increase the risk of vesicovaginal fistula formation [4]. Ureteral strictures are comparatively uncommon, occurring in 2.5% of patients who receive definitive radiation therapy. Strictures are typically managed with endoscopic procedures such as stent placement but may require more invasive, more permanent interventions. Perhaps the most important component of the management of ureteral strictures is to confirm that the stricture is not a recurrence by imaging [4]. Magnetic resonance imaging (MRI) is the optimal imaging modality for distinguishing cancer recurrence from radiation-related fibrosis such as strictures or fistulas [1]. To our knowledge, the presence of two of these rare complications of radiation therapy has not been widely described in the literature and only two case reports were identified that discuss a migrated ureteral stent through a cancer-related fistula.
A similar case in which a patient treated with surgery, chemotherapy, and radiation for squamous cell carcinoma of the cervix eight years prior to presentation had a displaced ureteral stent into the rectal lumen was reported in BioMed Central Urology [5]. The ureteral stent was placed for cervical cancer recurrence involving the right ureter with hydronephrosis [5]. She was treated with a combination chemotherapy regimen that included a vascular endothelial growth factor (VEGF) inhibitor to prevent angiogenesis of the tumor along with standard treatment with cytotoxic agents (cisplatin, paclitaxel) [5]. On admission, a sonography was performed for acute urinary tract infection and revealed bilateral hydronephrosis without visualization of the distal end of the stent in the bladder. Subsequent computed tomography (CT) showed the lower loop of the stent inside the rectum. Urinary fistulization was evidenced by the presence of iodinated contrast material in the rectal lumen. The fistulization was believed to be caused by necrosis of the pelvic tumor recurrence and increased wall fragility of the pelvic organs by the use of the VEGF inhibitor. The authors mention that they are aware of only one other reported case with a similar course [5]. That case describes an 85-year-old woman with a history of cervical cancer treated with hysterectomy and radiation 32 years prior to presentation for rectal bleeding who was found to have migration of a ureteral stent into the rectum discovered by colonoscopy [6]. In our case, the complications of metastatic cervical cancer and those of radiation therapy developed at different time intervals with the vesicovaginal fistula at diagnosis, ureteral stricture appearing two years after radiation, and the colovesical fistula after 10 years. The defects aligned perfectly to allow the ureteral stent to migrate outside of the body. In addition to these complications being relatively rare, the stent migration is even more so unexpected. Consideration of continued radiation-induced tissue damage should be included in patients with a history of pelvic radiation even in the absence of confirmatory imaging.
Conclusion
Pelvic radiation is often a necessary adjuvant treatment in patients with advanced gynecological cancers. The effects of radiation are caused by inflammation which can continue for decades after exposure. As cancer survivorship rates increase with improved treatments, it is important to anticipate continuing radiation damage in patients who have received radiation therapy two years prior.
REFERENCES
1.
Narayanan P, Nobbenhuis M, Reynolds KM, Sahdev A, Reznek RH, Rockall AG. Fistulas in malignant gynecologic disease: Etiology, imaging, and management. Radiographics 2009;29(4):1073–83. [CrossRef]
[Pubmed]

2.
Kim JH, Jenrow KA, Brown SL. Mechanisms of radiation-induced normal tissue toxicity and implications for future clinical trials. Radiat Oncol J 2014;32(3):103–15. [CrossRef]
[Pubmed]
3.
Emmert C, Köhler U. Management of genital fistulas in patients with cervical cancer. Arch Gynecol Obstet 1996;259(1):19–24. [CrossRef]
[Pubmed]
4.
Viswanathan AN, Lee LJ, Eswara JR, et al. Complications of pelvic radiation in patients treated for gynecologic malignancies. Cancer 2014;120(24):3870–83. [CrossRef]
[Pubmed]
5.
Tognarelli A, Faggioni L, Manassero F, Gadducci A, Selli C. A case report of endorectal displacement of a right ureteral stent following radiochemotherapy and Bevacizumab. BMC Urol 2019;19(1):128. [CrossRef]
[Pubmed]
6.
Billoud E, Savoye G, Hervé S, Ramirez S, Lerebours E. Double J ureteral stent as an unusual endoscopic finding in a patient with rectal bleeding. Gastrointest Endosc 2008;68(6):1239–40. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We would like to thank Dr. Olugbenga Oyesanmi for his contribution in technical editing and proofreading.
Author ContributionsJennifer Klein - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sunil Gandhi - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Jennifer Klein et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}