 |
Case Report
Biliary adenofibroma in a setting of primary biliary cholangitis and small duct destruction
1 Department of Pathology, The University of Texas Health Sciences Center at San Antonio, 7703 Floyd Curl Dr, San Antonio, TX 78229, USA
Address correspondence to:
Carlos Bouchot
MD, Department of Pathology, The University of Texas Health Sciences Center at San Antonio, 7703 Floyd Curl Dr, San Antonio, TX 78229,
USA
Message to Corresponding Author
Article ID: 100100Z11YK2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Trinidad C, Bouchot C, Sharkey F, Nazarullah A. Biliary adenofibroma in a setting of primary biliary cholangitis and small duct destruction. J Case Rep Images Pathol 2026;12(1):16–21.ABSTRACT
Biliary adenofibroma (BAF) is a very rare benign fibroepithelial neoplasm of the liver with the potential for malignant transformation. Most published cases present with either nonspecific clinical symptoms or are asymptomatic, typically with unremarkable laboratory findings. To the best of our knowledge, this is the first reported case of BAF in the setting of Primary Biliary Cholangitis (PBC). We present a finding of BAF in a 56-year-old woman with end-stage liver disease due to PBC. The explant liver showed a 2 cm area of distinct yellow-green nodularity in segments 7–8, with microscopic features diagnostic of BAF. We provide a comprehensive literature review of BAF, including characteristic histopathological findings of both benign and malignant forms, a review of pathogenesis, and a brief description of molecular and/or genetic alterations. These findings expand the clinicopathologic spectrum of BAF and underscore its occurrence in the setting of chronic cholestatic liver disease, with implications for recognition and assessment of malignant potential.
Keywords: Adenofibroma, Bile duct, Biliary, Liver, Neoplasm, Primary biliary cholangitis
Introduction
Initially described in the 1990s, biliary adenofibroma (BAF) is a rare, distinct, benign neoplasm of the bile ducts, with 55 cases reported [1],[2],[3],[4]. Its clinical significance is highlighted by its potential for malignant transformation. Grossly, BAF is often described as a well-circumscribed, cystic lesion. Histologically, it has two major components—proliferation of non-mucin-producing tubulocystic biliary duct epithelium and abundant fibroblastic stroma. A review of the literature reveals only one case of BAF in the setting of hepatic cirrhosis secondary to alcohol and hepatitis C infection [5]. We report a unique case of an incidental finding of BAF in association with primary biliary cholangitis (PBC) and bridging fibrosis in the explant liver of a 56-year-old woman. Additionally, we review histopathologic findings of both benign and malignant forms, examine the pathogenesis, and explore possible associations with PBC and duct plate malformations in the literature.
Case Report
The patient is a 56-year-old woman with hypertension who was diagnosed with anti-mitochondrial antibody (AMA)-negative PBC. She initially presented with fatigue and ascites. She had no history of hepatitis, excessive alcohol use, or familial liver disease. Liver function tests showed a cholestatic pattern, and a liver biopsy showed bridging fibrosis with rare plasma cells and focal lymphocytic infiltrates, suggestive of autoimmune cholangitis. A few years later, she had hematemesis due to esophageal varices which required banding. She underwent a transjugular intrahepatic portosystemic shunt (TIPS) procedure. She also underwent multiple paracentesis. She was placed on medications such diuretics and Ursodiol 300 mg thrice a day. However, her symptoms as well as her hepatic encephalopathy worsened over time. She was eventually diagnosed with end-stage liver disease. Imaging revealed end-stage cirrhosis without any masses or lesions. Liver transplant was then offered as intervention. She subsequently underwent a living donor liver transplant without intraoperative or postoperative complications.
Gross and Histopathologic Findings
The explant liver weighed 1067 grams. The external and cut surfaces were diffusely nodular, with nodules ranging from 0.1 to 0.7 cm. In segments 7–8, there was a 2 × 0.7 × 0.5 cm area with distinct yellow-green cut surface. No other distinct nodules, lesions, or masses were seen.
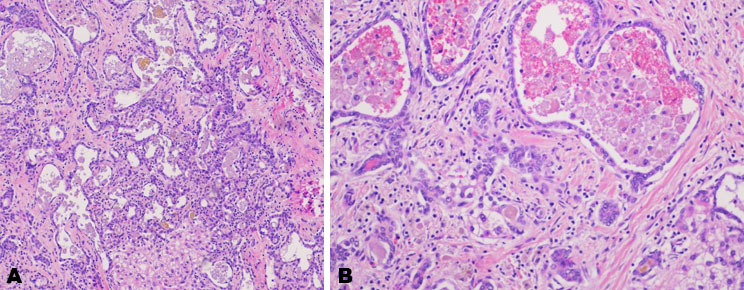
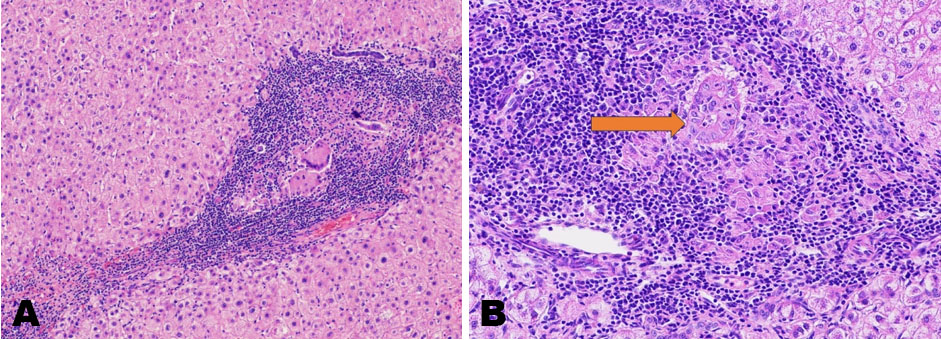
Microscopic examination of the nodular lesion showed a tubular and microcystic proliferation of low-grade biliary epithelium embedded in a cellular fibrous stroma. The proliferation spread out from a central core along fibrous bands, focally resembling bile ductules filled with bile and other debris (Figure 1A and Figure 1B).
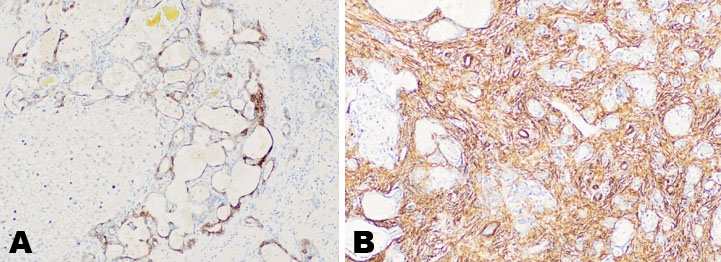
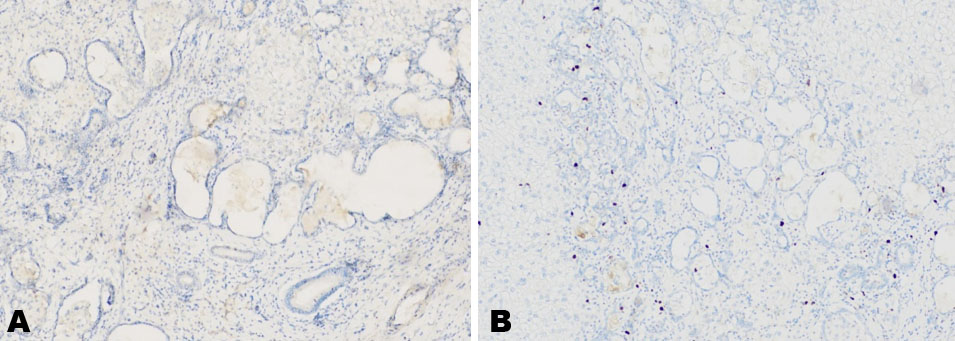
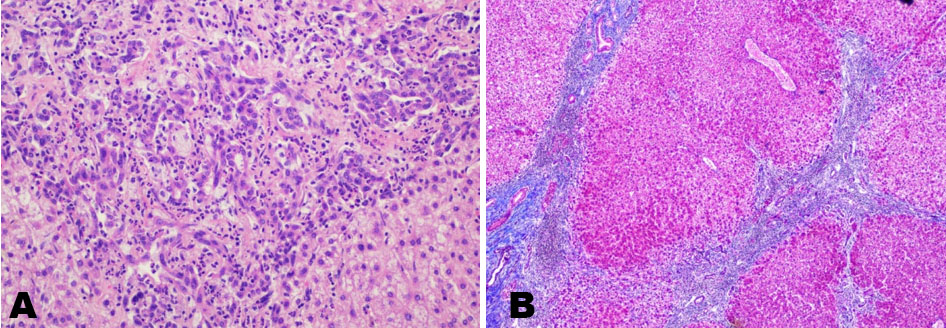
Immunohistochemical stains showed that KRT7 (Cytokeratin 7) highlighted the epithelial component of the neoplastic cells, while Smooth Muscle Actin (SMA) was positive in the surrounding stroma (Figure 2A and Figure 2B). The following immunohistochemical stains were negative: KRT20 (Cytokeratin 20) and Napsin. p53 was wild type. Ki-67 proliferation index was low at less than 5% in the lesional epithelial cells (Figure 3A and Figure 3B).
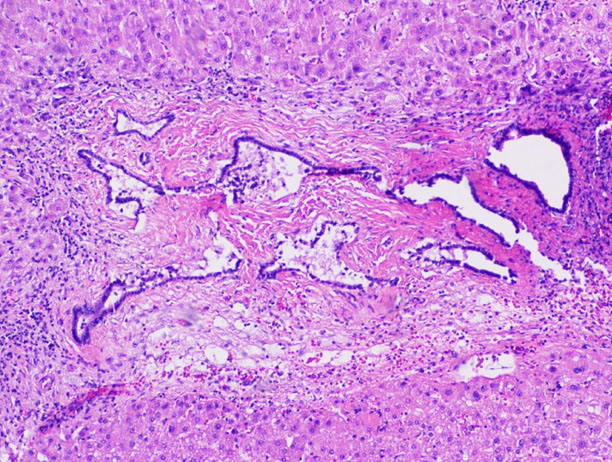
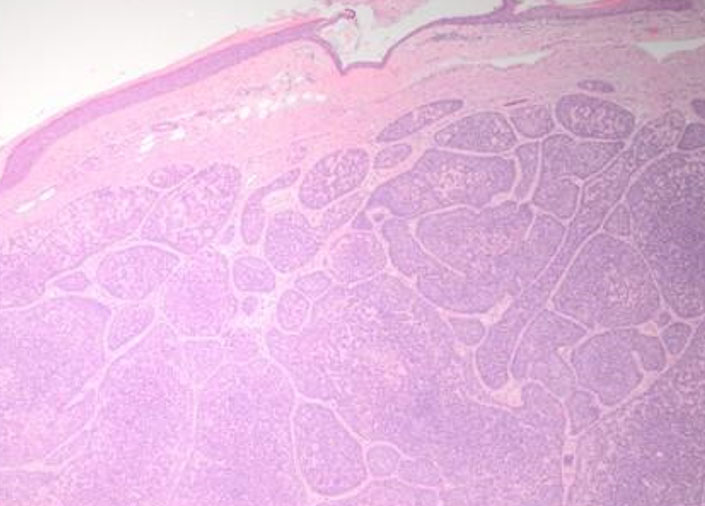
Two other smaller lesions consistent with bile duct hamartoma (von Meyenburg complex) were found in the specimen, separate from the larger lesion (Figure 4).
The background liver parenchyma displayed biliarytype bridging fibrosis (Stage 4, assessed using Trichrome stain, Figure 5) with narrow fibrous bands, some of which contained occasional medium-sized bile ducts. The interlobular bile ducts were predominantly absent; however, proliferative ductules were seen (Figure 6). There were nodular aggregates of lymphocytes present in the fibrous bands (Figure 5). A couple of portal tracts had lymphohistiocytic infiltrates. There was very minimal macrovesicular steatosis (<1%). The overall morphology supported the clinicopathologic setting of AMA-negative PBC.
Discussion
Biliary adenofibroma is a rare liver lesion, first reported in 1993 by Tsui et al. as a distinct biliary neoplasm with a striking resemblance to von Meyenburg complex (biliary hamartoma). Although von Meyenburg complexes may share some overlapping histologic features with biliary adenofibroma, several features in our lesion support classification as BAF. The lesion measured 2 cm, exceeding the typical size of hamartomas (
The WHO in 2010 classified BAF as a benign entity arising from the bile ducts. However, this lesion has potential for malignant transformation. Complete surgical resection is curative in benign BAF, whereas malignant cases may recur locally or metastasize [3].
Hu et al. reviewed 27 reported cases of BAF, 12 of which displayed malignant transformation [3]. In a detailed clinicopathologic analysis, the 27 patients (12 males and 15 females) had ages ranging from 23 to 83 years and exhibited unremarkable physical examination and laboratory findings. The vast majority were either asymptomatic or reported right upper quadrant abdominal pain. Only one case, originally reported by Meguro et al. [5], had a background of liver cirrhosis, and was associated with alcohol and hepatitis C. A few of the malignant cases reviewed by Hu et al. also had histologically benign areas, which also showed lower Ki-67 proliferation index by immunohistochemistry. The Ki-67 proliferation index in malignant areas was at least 20% [3]. Three of the 27 cases from the same paper were reported to also have von Meyenburg complexes separate from the BAF. Our review of the literature did not identify any case of BAF associated with PBC or other bile duct-based disease, making this report the first to describe BAF in the setting of PBC and/or primary ductal disease in the literature.
Biliary adenofibroma has been grossly described as well-circumscribed and tan white, with small cystic spaces [4]. Meguro et al. [5] described one case with underlying liver cirrhosis in which the lesion underwent malignant transformation. This lesion measured 3 cm, was well-circumscribed with a solid and microcystic cut surface and showed necrosis and invasion into the main portal vein. In a benign case without background liver disease or cirrhosis in a 79-year-old patient, reported by Gurrera et al., the lesion was described as a 5.5 cm nodular, well-circumscribed, firm mass, with a solid and microcystic appearance [6].
Biliary adenofibroma is characterized microscopically by proliferation of non-mucin secreting tubulocystic structures variably embedded in a fibrous stroma [7]. Its immunophenotypic profile suggests that it is of large bile duct and/or interlobular duct origin [6]—i.e., positive for KRT7, KRT8, KRT18, KRT9, and CD10. In a 2003 report [8], benign biliary adenofibroma was characterized by two distinct components: cystic and tubular structures lined by low columnar to cuboidal biliary-type epithelium, and a dense fibrous stroma composed of spindle-shaped cells with mild nuclear pleomorphism and inconspicuous nucleoli. In a benign case published in 2003 [8], the lesion was described with two distinct components—cystic and tubular structures lined by low columnar to cuboidal biliary-type epithelium, and a dense fibrous stroma with spindle-shaped cells with mild nuclear pleomorphism and inconspicuous nuclei. There were no mitotic figures or stromal invasion. Our report describes a well-circumscribed 2 cm lesion with low-grade biliary epithelium with a tubular and microcystic appearance in a cellular fibrous, consistent with known characteristics of benign BAF. Mitotic figures, stromal invasion, and marked cellular atypia were absent, supporting the benign nature of this tumor.
Histologic Characteristics of Malignant Transformation
In the detailed analysis published by Hu et al. [3], malignant transformation was described as having the following histological characteristics—disordered polarity, elongated hyperchromatic vesicular nuclei with prominent nucleoli, atypical mitotic figures, complex architecture (papillary, cribriforming, back-to-back glands), lymphovascular, stromal, perineural, and/or liver capsule invasion, all of which suggest transformation to cholangiocarcinoma. Cholangiocarcinoma is an aggressive epithelial cell malignancy with features of cholangiocyte differentiation and can occur along the biliary tree and/or within the hepatic parenchyma [9].
As an example of these features, the case published in 2016 by Godambe et al. [10] described a definite malignant component with infiltrative borders, liver capsule invasion, and penetration into surrounding adhesions and skeletal muscle. Immunohistochemical studies further supported the malignant component in this case—i.e., p53 showed moderate (25–50%) positivity (aberrant staining) and Ki-67 was uniformly brisk in the ductular component. In contrast, immunohistochemistry stains in our patient supported a benign nature, i.e., Ki-67 proliferation index was low at 5%, and p53 was wild type.
In a study by Liao et al. [11], BAF has been recognized as a potential precursor lesion for intrahepatic cholangiocarcinoma, and they suggest that it is part of a continuum of tumorigenesis. In contrast to our case, the tumors reported in their study exhibited malignant histologic features, such as infiltrative growth pattern, higher degree of nuclear atypia, complex architecture, and lymphovascular invasion.
Molecular and Genetic Alterations
In a study of six cases [12], there was no unifying pathogenic mutation or genomic alteration specific to BAF. Although abnormal p53 nuclear accumulation was observed by immunohistochemistry in the two cases that they reported, no p53 gene mutation was identified. IDH1 gene mutation that is seen in 25% of cholangiocarcinomas was not present [12].
Several studies performed on cases with malignant transformation have shown mutations associated with aggressive behavior [13] and with other human cancers such as cholangiocarcinoma [11],[14],[15]. These include mutations in ARID1A, BAP1, PBRM1, IDH2, TP53, and FGFR2 [2],[11].
Primary Biliary Cholangitis and Biliary Adenofibroma
This case was especially unique, given that this bile duct neoplasm arose in a background of PBC, a disease-causing destruction of small bile ducts. Primary biliary cholangitis has not previously been reported in association with BAF. It is an autoimmune-mediated disease characterized by progressive granulomatous destruction of small to medium-sized interlobular and septal intrahepatic bile ducts [16]. There is a female-sex predominance and association with anti-mitochondrial (AMAs) and disease-specific antinuclear antibodies (ANAs). There is a characteristic T-cell-mediated destruction of small bile duct epithelial cells, leading to ductopenia, persistent cholestasis, and eventually, end-stage liver failure [17]. Notably, a pathognomonic sign of PBC in histology is interlobular bile duct destruction [18]. This case raises the possibility that chronic bile duct injury may create a microenvironment for aberrant ductular proliferation and neoplastic transformation. Alternately, coexistence may be incidental. Further studies are needed to determine whether PBC confers any predisposition to biliary neoplasms like BAF.
Although multiple benign liver neoplasms like biliary adenoma, hepatocellular adenoma, hemangioma, and focal nodular hyperplasia have been described in settings of PBC, they do not have increased risk of occurrence in PBC settings compared to baseline population. On the other hand, patients with PBC have increased risk of malignancies like cholangiocarcinoma and hepatocellular carcinoma. Developmental/ductal plate malformations such as biliary hamartomas (von Meyenburg complexes) are also incidentally found in livers with PBC and is also thought to have no definite pathogenic association with PBC.
Biliary adenofibroma has some morphologic overlap with bile duct hamartoma but they are larger in size with a more complex epithelial component and cellular stroma [1]. Bile duct hamartomas are congenital malformations of the interlobular bile ducts, caused by lack of embryonic involution [19]. Since BAF appears to arise from interlobular bile ducts, and based on its immunophenotypic profile [6], one might speculate that BAF may initially arise as a congenital malformation before acquiring additional genetic changes causing its development into a neoplasm. This has been explored further by a study where intrahepatic cholangiocarcinoma associated with BAF and ductal plate malformations show a similar spectrum of molecular alterations, notably ARID1A loss [11].
Conclusion
This represents the first reported case of biliary adenofibroma arising in the setting of primary biliary cholangitis. Although no definitive pathogenic association between these entities has been established, this is a unique association of a benign neoplasm arising in a background of ductopenia and bile duct destruction. The recognition of biliary adenofibroma is important to avoid misdiagnosis as cholangiocarcinoma, particularly in patients with PBC who are at increased risk for malignancy. Despite its benign classification, biliary adenofibroma has recognized potential for malignant transformation, underscoring the importance of accurate diagnosis and awareness of its clinicopathologic features.
REFERENCES
1.
Tsui WM, Loo KT, Chow LT, Tse CC. Biliary adenofibroma. A heretofore unrecognized benign biliary tumor of the liver. Am J Surg Pathol 1993;17(2):186–92.
[Pubmed]

2.
Mattiolo P, Zen Y, Zhang X, Scarpa A, Luchini C, Graham RP. Biliary adenofibroma and cholangiocarcinoma: Neighbors or relatives? A systematic and critical review. Hum Pathol 2025;165:105872. [CrossRef]
[Pubmed]
3.
Hu W, Zhao Y, Liu Y, Hua Z, Liu A. Imaging features of biliary adenofibroma of the liver with malignant transformation: A case report with literature review. BMC Med Imaging 2022;22(1):47. [CrossRef]
[Pubmed]
4.
Alshbib A, Grzyb K, Syversveen T, Reims HM, Lassen K, Yaqub S. Biliary adenofibroma: A rare liver tumor with transition to invasive carcinoma. Case Rep Surg 2022;2022:5280884. [CrossRef]
[Pubmed]
5.
Meguro S, Yamazaki S, Matsushima S, Kawata K, Kawasaki H, Tsuchida T, et al. A case of a primary hepatic so-called adenosarcoma with heterotopic ossification: Possibly of biliary adenofibroma origin. Hum Pathol 2018;73:108–13. [CrossRef]
[Pubmed]
6.
Gurrera A, Alaggio R, Leone G, Aprile G, Magro G. Biliary adenofibroma of the liver: Report of a case and review of the literature. Patholog Res Int 2010;2010:504584. [CrossRef]
[Pubmed]
7.
Nguyen NTT, Harring TR, Holley L, Goss JA, O’Mahony CA. Biliary adenofibroma with carcinoma in situ: A rare case report. Case Reports Hepatol 2012;2012:793963. [CrossRef]
[Pubmed]
8.
Varnholt H, Vauthey JN, Dal Cin P, Marsh Rde W, Bhathal PS, Hughes NR, et al. Biliary adenofibroma: A rare neoplasm of bile duct origin with an indolent behavior. Am J Surg Pathol 2003;27(5):693–8. [CrossRef]
[Pubmed]
9.
Brindley PJ, Bachini M, Ilyas SI, Khan SA, Loukas A, Sirica AE, et al. Cholangiocarcinoma. Nat Rev Dis Primers 2021;7(1):65. [CrossRef]
[Pubmed]
10.
Godambe A, Brunt EM, Fulling KH, Reza Kermanshahi T. Biliary adenofibroma with invasive carcinoma: Case report and review of the literature. Case Rep Pathol 2016;2016:8068513. [CrossRef]
[Pubmed]
11.
Liao X, Agostini-Vulaj D, Li RX, Zhang X. Characterization of cholangiocarcinomas with tubulocystic morphology associated with biliary adenofibroma or biliary adenofibroma-like lesions. Mod Pathol 2025;38(10):100815. [CrossRef]
[Pubmed]
12.
Borger DR, Tanabe KK, Fan KC, Lopez HU, Fantin VR, Straley KS, et al. Frequent mutation of isocitrate dehydrogenase (IDH)1 and IDH2 in cholangiocarcinoma identified through broad-based tumor genotyping. Oncologist 2012;17(1):72–9. [CrossRef]
[Pubmed]
13.
Arnason T, Borger DR, Corless C, Hagen C, Iafrate AJ, Makhlouf H, et al. Biliary adenofibroma of liver: Morphology, tumor genetics, and outcomes in 6 cases. Am J Surg Pathol 2017;41(4):499–505. [CrossRef]
[Pubmed]
14.
Thompson SM, Zendejas-Mummert B, Hartgers ML, Venkatesh SK, Smyrk TC, Mahipal A, et al. Malignant transformation of biliary adenofibroma: A rare biliary cystic tumor. J Gastrointest Oncol 2016;7(6):E107– 12. [CrossRef]
[Pubmed]
15.
Jiao Y, Feng Y, Wang X. Regulation of tumor suppressor gene CDKN2A and encoded p16-INK4a protein by covalent modifications. Biochemistry (Mosc) 2018;83(11):1289–98. [CrossRef]
[Pubmed]
16.
Reshetnyak VI. Primary biliary cirrhosis: Clinical and laboratory criteria for its diagnosis. World J Gastroenterol 2015;21(25):7683–708. [CrossRef]
[Pubmed]
17.
Lleo A, Invernizzi P, Mackay IR, Prince H, Zhong RQ, Gershwin ME. Etiopathogenesis of primary biliary cirrhosis. World J Gastroenterol 2008;14(21):3328–37. [CrossRef]
[Pubmed]
18.
Lleo A, Marzorati S, Anaya JM, Gershwin ME. Primary biliary cholangitis: A comprehensive overview. Hepatol Int 2017;11(6):485–99. [CrossRef]
[Pubmed]
19.
Sheikh AAE, Nguyen AP, Leyba K, Javed N, Shah S, Deradke A, et al. Biliary duct hamartomas: A systematic review. Cureus 2022;14(5):e25361. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Camille Trinidad - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Carlos Bouchot - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Francis Sharkey - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Alia Nazarullah - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Camille Trinidad et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}